OACIS was founded on a simple observation: as payers, EHR vendors, and RCM platforms become increasingly automated, the practices that will struggle most are not those with poor technology — they are those without a partner who genuinely owns their revenue performance.
Accelerate Every Dollar. Reduce Revenue Leakage.
From patient access to final payment — OACIS owns every stage of your revenue cycle.
The industry is changing
Revenue cycle management is evolving — and most practices aren't keeping up
2005
Billing Era
Paper to electronic claims
The primary challenge was digitizing the billing process. Human data entry was the core function. Claims were submitted manually and followed up by phone. One biller could manage a small practice.
2015
EHR Era
Practice management integration
EHR systems began incorporating billing functionality. Eligibility checks, claim generation, and basic denial reporting became integrated. RCM companies grew larger and began serving thousands of clients simultaneously.
2022
Automation Era
AI enters the revenue cycle
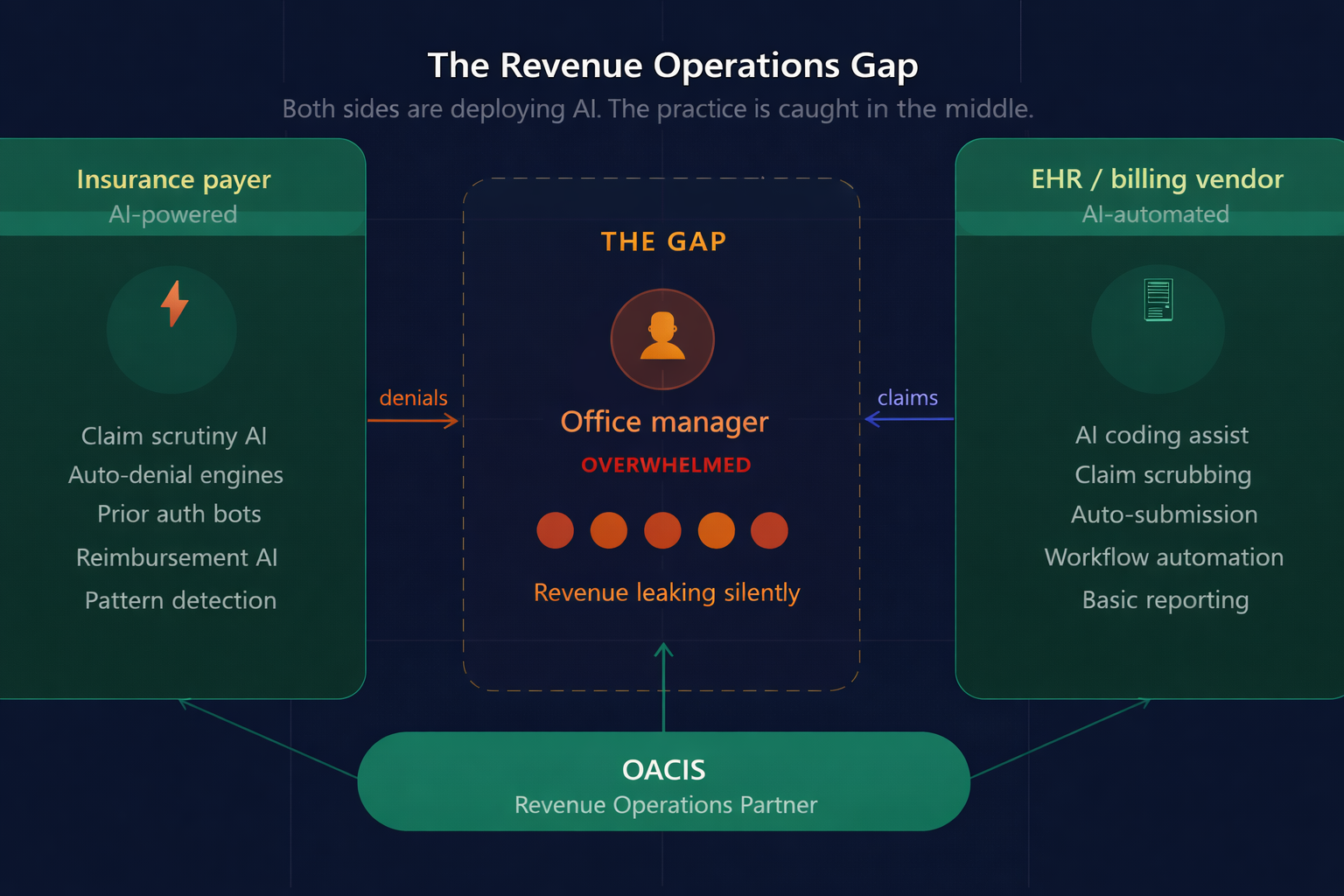
Both payers and EHR vendors began deploying AI. Coding assistance, automated claim scrubbing, and predictive denial tools became standard offerings. Large RCM vendors began reducing staff while serving more clients. Response times lengthened. Ownership became diluted.
Now
REVENUE OPR Era
The challenge is no longer submitting claims
AI automates routine tasks on both sides — payers and providers. The practices that will thrive are not those with better billing software. They are those with a Revenue Operations partner who combines AI efficiency with genuine human accountability. That is OACIS.
Across multiple revenue cycle audits of independent healthcare practices, a pattern emerged that had nothing to do with billing software, coding accuracy, or claim submission speed.
Practices were submitting claims. Payments were arriving. Reports were being generated. And yet revenue was quietly declining — through denials nobody followed up on, underpayments nobody identified, and A/R that kept aging without anyone owning it.
When we asked these practices who was responsible for resolving reimbursement issues, the answer was almost always the same: nobody had a clear answer.
That’s the problem OACIS was built to solve. Not billing. Revenue ownership.
"We thought we had a billing problem. What we really had was a revenue ownership problem. Claims were going out — but nobody was watching what came back, why things were denied, or what we were leaving on the table." — Observation from urgent care revenue operations audit
What we consistently found
A/R aging without systematic follow-up
Three questions that shaped OACIS
These are the questions we kept asking — and that most practices couldn't clearly answer — during our revenue cycle audits of independent healthcare organizations.
How confident are you that you're collecting every dollar you're entitled to today?
Most practices can tell us how many claims were submitted. Very few can tell us where revenue is being delayed, denied, underpaid, or lost.
If collections started declining next month, would you know exactly why?
The practices that answer this confidently have revenue intelligence. The ones that don't have a billing vendor. There's a significant difference.
Who owns the outcome when a reimbursement problem arises?
Not who processes the claim. Not who generates the report. Who picks up the phone, escalates to the payer, and stays with it until the issue is resolved?
How OACIS differs from large EHR + RCM vendors
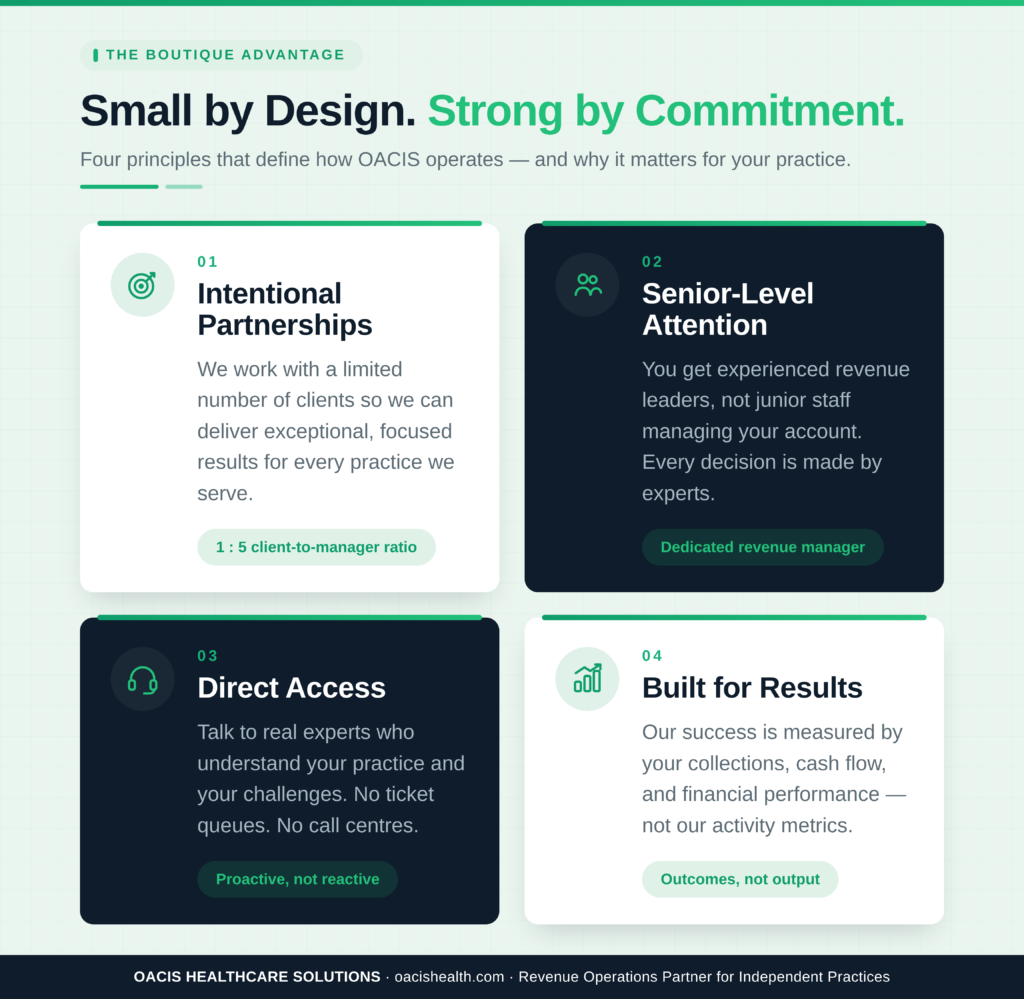
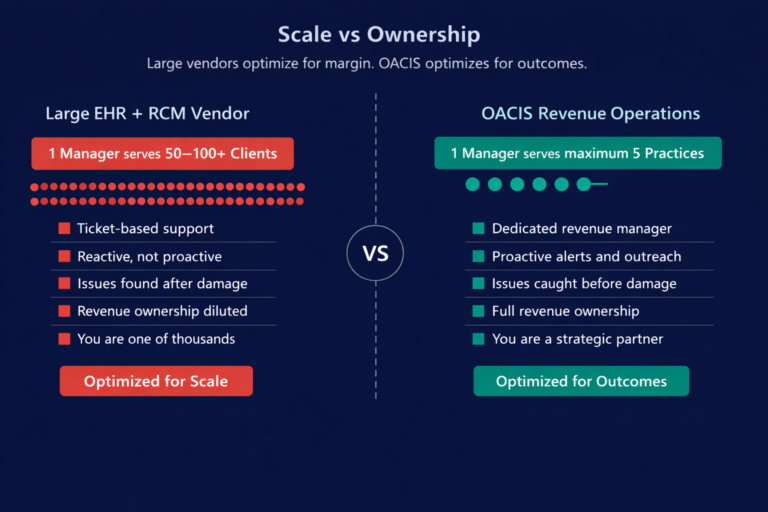
Large EHR + RCM platforms are excellent at what they're built for: scale, automation, and standardization. OACIS is built for something different: accountability, intelligence, and financial ownership for independent practices.
How OACIS differs from large EHR + RCM vendors
Large EHR + RCM platforms are excellent at what they're built for: scale, automation, and standardization. OACIS is built for something different: accountability, intelligence, and financial ownership for independent practices.
A free 30-minute Revenue Operations Review identifies exactly where collections are being delayed, denied, or lost — and what a realistic improvement looks like.
Patterns we see again and again across independent practice revenue cycles.
The OACIS Healthcare team demonstrated a strong understanding of urgent care revenue cycle complexity and brought a level of operational insight that went far beyond traditional billing discussions. Their structured audit identified several revenue leakage patterns and meaningful operational and financial optimization opportunities that were not previously visible to our team.
We frequently begin audits at practices running denial rates near 20%, with no payer-specific workflow behind their billing. The denials are overwhelmingly preventable — eligibility gaps, missing authorizations, and modifier errors — and a disciplined, payer-specific process is what separates a sub-5% denial rate from a 20% one.
Claim rejections in the low double digits are common in practices without a structured front-end review. In our experience, the issue is almost never coding talent — it's the absence of a consistent guideline system. Once one is in place, rejections and denials typically fall sharply within the first two months.
A recurring red flag we document is A/R over 90 days sitting well above benchmark — often a quarter or more of total receivables — while net collection rates quietly underperform. Aging A/R is the clearest early signal that follow-up has no owner, and it's usually the fastest place to recover real dollars.
Out-of-network and non-par claims are where we see the most revenue left on the table. Without a deliberate strategy for timely filing and payer negotiation, low reimbursements get accepted as final and written-off balances go unrecovered — when many are, in fact, collectible with the right approach.